I have a confession. I work at the Greenwood Genetic Center, but I do not have a background in science; marketing is more my speed.
It would be an understatement to say that, since working at GGC, I’ve gained new perspectives (I’m talking about you, insurance) and have learned A LOT about genetics. I mean, I didn’t completely sleep through biology class and remember things like humans have 46 chromosomes, A goes with T and C goes with G, mitochondria are the powerhouse of the cell, and so on. But like GGC’s Biochemical Lab Supervisor, Teresa Thompson, I had no idea biochemical genetics existed—and she was a science major!
Teresa’s career at GGC began with an internship during her senior year at Erskine College. After graduation, she worked at an environmental lab but was so eager to join GGC that she volunteered in the research lab two nights a week and for a few hours on Saturdays until her first child was born in 1999. She kept in touch, and GGC co-founder Dr. Hal Taylor hired her in 2000 as the primary biochemical technologist performing biochemical tests.
in the research lab two nights a week and for a few hours on Saturdays until her first child was born in 1999. She kept in touch, and GGC co-founder Dr. Hal Taylor hired her in 2000 as the primary biochemical technologist performing biochemical tests.
So, let’s get to the nerdy— I mean, fun— stuff.
What is biochemical genetics?
Laura Pollard, PhD, Lead Director of GGC’s Biochemical Lab, says, “In its simplest form, biochemical genetics refers to the diagnosis and monitoring of patients with inborn errors of metabolism, which are genetic disorders that inhibit a specific metabolic pathway in the body like those required to break down proteins, fats/lipids, or sugars.”
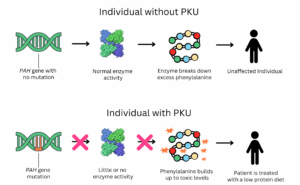
A good example is the amino acid disorder phenylketonuria (PKU). Individuals with PKU cannot fully break down protein due to a change in the PAH gene. This gene provides instructions for the body to make phenylalanine hydroxylase, the enzyme that breaks down the amino acid phenylalanine. Amino acids are the building blocks of protein, and when this enzyme is not functioning correctly, phenylalanine can build up to toxic levels.
I don’t have children, so I’m not familiar with the newborn stage. In fact, newborns scare me. But one of the first things I learned when I started working at GGC was about newborn screening.
Newborn screening is a test conducted shortly after birth to identify conditions that may not be immediately apparent but could affect the child’s long-term health if left undiagnosed or untreated. PKU was the very first genetic disorder that was screened for in newborns starting in the mid-1960s. If PKU is untreated, toxic levels of phenylalanine can accumulate, which can lead to seizures, intellectual disability, and psychiatric symptoms. If a newborn is diagnosed with PKU, treatment, in the form of a special medical formula that is low in phenylalanine, is begun right away to prevent the toxic buildup and help avoid these serious complications.
What is GGC’s role in newborn screening? All infants born in South Carolina have their heel pricked before they leave the hospital. Five drops of blood are collected on a dried blood spot (DBS) card, which is then sent to the state lab in Columbia, SC for screening. If the state lab determines that additional testing is needed, the same DBS card is sent to the biochemical lab at GGC. Within 24 hours of arriving at GGC, the results are given to the baby’s physician, and the GGC clinical metabolic team is notified. Together with the family, a treatment plan is initiated.
When Teresa was the primary technologist, you can imagine the urgency she felt to complete the lab work. It was a very manual process back then, and the results from the thin-layer chromatography technology were qualitative. Teresa and the lab director had to compare the patient’s banding patterns to controls to confirm or rule out the suspected condition. Since the lab adopted mass spectrometry in 2005, the process has become less manual and now provides quantitative data, offering families definitive positive or negative results. Mass spectrometry not only benefits South Carolina’s newborn screening program but also patients all over the world.
Other metabolic conditions like mucolipidosis, Sanfilippo syndrome, Krabbe disease, and other lysosomal storage disorders are so rare, only a few premier laboratories like the biochemical lab have expertise in performing these tests. GGC’s diagnostic lab has a long history of collaborating with pharmaceutical companies on clinical trials for confirming patient diagnoses and analyzing biomarkers which help tell us if a treatment is working.
If you have been following these monthly ‘Then and Now’ posts, you have probably noticed a trend: GGC employees tend to stay at GGC for a long time. Each month, I look forward to asking the question, “What is your favorite part of your job and what has kept you at GGC for so long?” Teresa shared her love of science and how genetics has always fascinated her. She appreciates that, despite the constant innovation at GGC, the mission has always remained the same – helping patients. And her favorite part of her job? Confirming a diagnosis that will determine how to treat a patient.
As we were talking, I could see the passion Teresa has for her work, and I even gained a new perspective during our conversation (and it isn’t about insurance). Back when she was still the primary biochemical technologist, she had to stay late at work quite a bit, even with a new baby at home. Her husband asked why one day, and she replied, “I would want someone staying late in the lab if our baby needed a diagnosis in order to get help.”
If I ever have a child who needs a diagnosis, I would want someone like Teresa working in the lab.
Post by Caroline Pinson